Total Knee Replacement
Indications for Total Knee Replacement
There are a variety of conditions which may result in a worn-out knee joint. Most common is osteoarthritis, a “wear-and-tear” condition in which the protective cartilage covering of the joint gradually thins out over time, resulting in progressive knee pain and stiffness.
More rarely seen are the inflammatory types of arthritis, such as rheumatoid arthritis, which is a medical condition resulting in progressive cartilage loss.
Previous injury or deformity to the knee or limb results in changes to the local biomechanical properties of the knee joint, which may accelerate cartilage loss.
When the joint damage has become sufficiently severe, and the patient’s quality of life is beginning to suffer, a total knee replacement may be indicated.
Historical Perspective
Total knee replacement surgery is a highly successful procedure for eliminating the pain and stiffness associated with knee arthritis. Most simply put, this procedure involves removing the damaged cartilage and bone from the inside of the knee and then replacing the weight-bearing surfaces with a new implant (similar to capping a tooth) that allows a smooth arc of motion and the ability to walk without pain.
Over time, the surgery techniques, implants, and instrumentation have continued to evolve in order to improve patient outcomes. Ensuring that a patient undergoing this surgery will have a good result requires careful attention to the patient’s limb alignment and meticulous handling of the soft tissues.
Surgical Technique
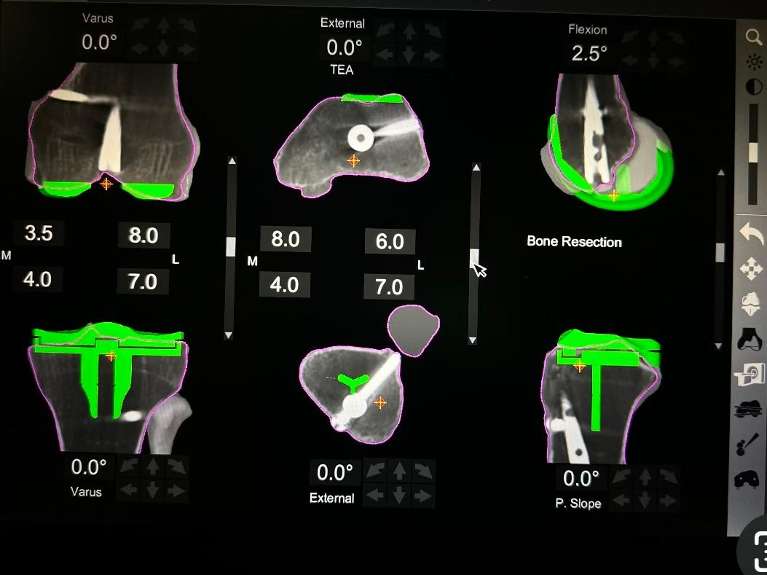
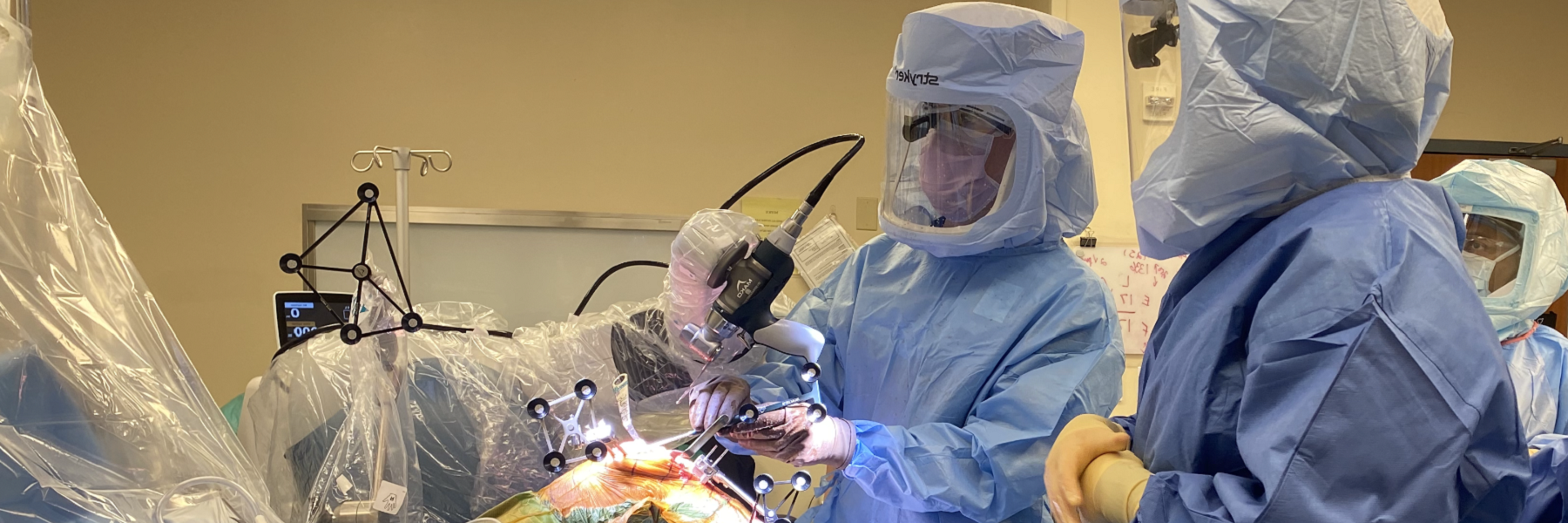
During a knee replacement, the surgeon designs the space between the tibia and femur to be an equal, rectangular “gap” in both flexion and extension, prior to finishing bone preparation and inserting the implants. This involves releases of ligaments that are too tight, resection of bone spurs which can alter the knee balance, and adjusting the rotational alignment of the femoral component so that it parallels the plane of the tibial component. Using robotic arm assistance or computer navigation increases the accuracy and precision of component implantation.
A well gap-balanced surgery ensures that the patient’s knee feels equally stable in both flexion and extension, and the patella tracks normally throughout the arc of motion.
Post-Operative Recovery
After a total knee replacement, patients may immediately weight bear as tolerated, with no restrictions. The range of motion of the knee is progressively improved over the first few weeks. Specific physical therapy protocols are available on the website and will be initiated by your physical therapist.
For the first 2-4 weeks, patients are encouraged to walk, practice going up and down stairs, and generally resume the activities of daily living.
By 2-4 weeks, most patients have discontinued the need for a cane and are walking unsupported.
From 6-12 weeks, the patient will notice larger gains in physical therapy in terms of endurance, the range of motion, and strength.
Usually, by 12 weeks, the patient is starting to feel close to normal and is resuming most activities, but many patients continue to see ongoing improvement even up through one year after surgery.